


Clinical Inquiry Fellowship - getting started
Foundations and applications from a DPT program to a fellowship

Clinical Inquiry is not just what I teach. It has been a career long process for me - dating back to when I was a PT student in 1992. I’ve told the story before - but basically I got a bad answer to one of my questions and I thought it should be better.
I can’t claim that my thinking has always been productive, or even coherent; but I can say that it has been a long slow journey in the same direction (keeping in mind that you can travel hundreds of miles “in the same direction” despite doing several individual miles in opposite directions - - it’s not the most efficient way to get somewhere, but it gets you there).
I want to first share what I’ve figured out as two possible starting points for a Clinical Inquiry Fellow (CIF). These are not the only two starting points, but they are where I am right now in terms of my thinking. Which starting point any particular CIF takes is up to them.
One Approach: Start with Critical Realism
One is with Critical Realism - to say my reading and thinking in this area has had a huge impact on me would be an understatement. My thinking about critical realism started in 1994, and like many things it was before I knew what I was doing. I was a student on a clinical rotation in Florida in July. Needless to say - I couldn’t go outside. I was living alone. I had a lot of free time. I was reading a paper on the Disablement Process by Alan Jette, it was published in May 1994 and I took the journal with me to Florida for reading.
The paper did not refer to Critical Realism (CR) and subsequent papers about this process in the PTJ were highly influenced by the more empirically (ontologically anbd epistemologically) restricted scientific realism. But the paper really should be seen through a CR lens.

I saw figure 2 and realized I was in a profession that spanned a rather broad stratification of reality (didn’t use those words - learned them later when learning about CR), and that stratification of reality meant it would be important to consider the ontology of each strata, which then influenced what and how we can know, the epistemology. Again, I had no idea what the words were for what I was thinking about - that would take about 12 more years).
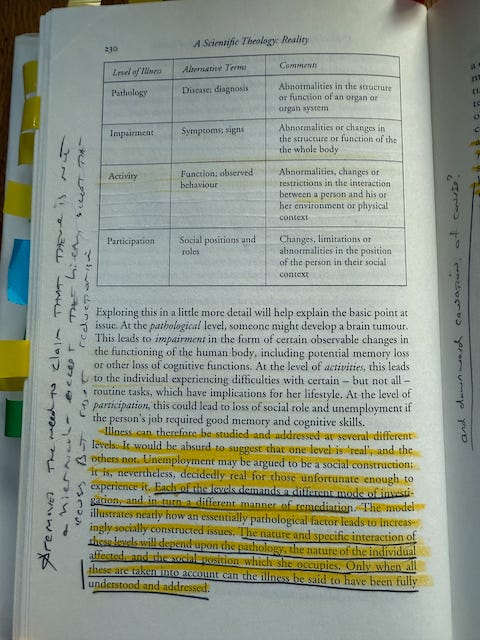
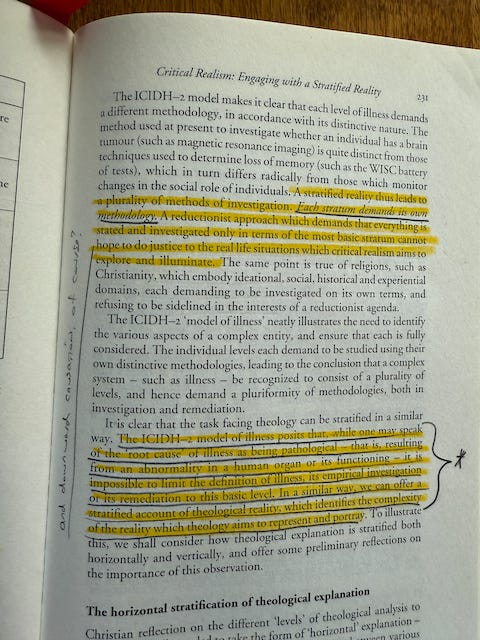
Flashforward to 2006, I was reading McGrath’s “A Scientific Theology: Volume 2: Reality” and low and behold, McGrath used the disablement model as a way to describe illness through the lens of Bhaskar’s Critical Realism.
To say I was excited is an understatement. I had been reading along about “Engaging with a Statified Reality” and the disablement model example appeared!

There are many routes to understanding CR; but the fact is - most of the important concepts are very well understood by physical therapists, we just lack the language to articulate the ideas and discuss their implications and applications. What I’ve found is that the challenges many PTs face is that they are critical realists, but they are living in a world that is made up of many logical positivists or otherwise extreme empiricists. The problem is further compounded by the fact that even the logical positivists and extreme empiricists cannot sustain those positions and function in our world.
I could go on, and at some point in some format, I will. But CR is critical (pun intended) to clinical inquiry. It is the philosophical foundation of clinical inquiry; and it is what I had in mind for the PSU DPT program and now have in mind for the clinical inquiry fellowship.
DPT Program Philosophy
The DPT Program embraces a critical realist philosophy of science and its associated consequences that ontology determines epistemology and the stratification of reality. We fully support the use of evidence-based empirical observations in the development of knowledge, and the subsequent rationale development of knowledge for use in practice, a framework we describe as knowledge-based practice. We believe the best representations of knowledge for practice are causal structures, including models and networks from which logical inferential rules can be applied in clinical decision-making.
As a fellow - one way to start is to learn about Critical Realism - engage with it for a bit and think about what it means.
I said there were two possible ways to get started. CR is one way. With it you’re ready for the next step through the CR lens. And that’s useful.
Another Approach: Start with Logic
Another useful approach (note, not second or inferior, just different) is to start with logic and by logic I mean all forms of logic - the formal approach of deduction with it’s valid forms and sound conclusions to the ampliative logics of induction and abduction. It turns out they all require an understanding of probability (and set theory), and they are wonderful tools for the application of a CR approach. In clinical inquiry (1) I teach three forms of logical inference and their associated probability:
Logic. Inference. Related use of probability
Deductive. Deduction. Probability logic (conditional probabilities)
Inductive. Induction. Statistical inference.
Abductive. Abduction. Bayesian inference.
To apply these forms of inference to practice we must embrace uncertainty (which is where the associated probabilities help), and we apply them to causal inferences (because all clinical reasoning is based on causation).
Here’s the model I had in mind back then -
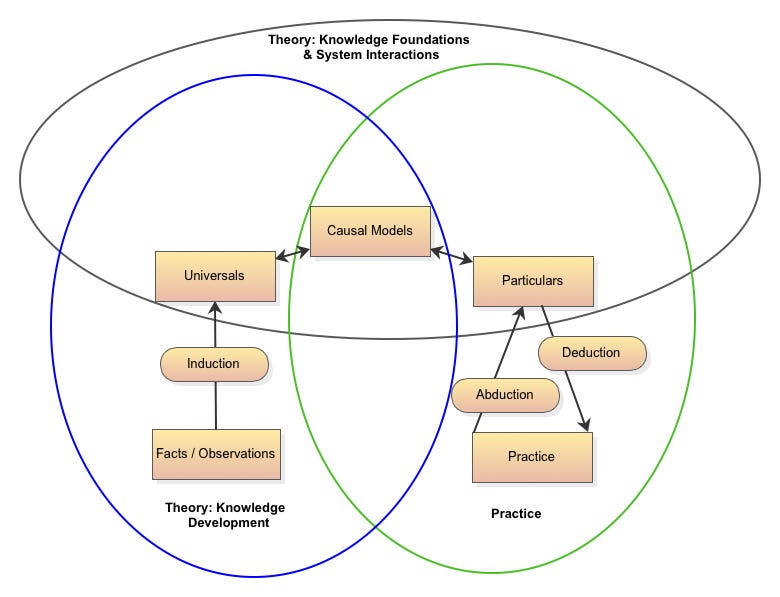
Here - causal models form the “knoweldge” from which we practice and the bridge from which universals (ontological realities) bring understanding to situations.
After both Critical Realism and Logic -
Therefore, Once you understand CR; and Logic (as described above), I think it’s time to start thinking about applying them to understanding causation within the clinical process (i.e. doing and reasoning); meaning, doing clinical inquiry. And either while - or after - learning about causation, it’s time to remind yourself of all the ways our thinking can go wrong (bias and fallacies).
I’m still not sure how much of what I teach in Clinical Inquiry 1 sticks. But I’m confident that anyone willing to take on the challenge of being a Clinical Inquiry Fellow will be prepared to make some contributions, and at the very least, will have a better understanding of the problems within the profession and possibly - - how to contribute to solutions.
Let me know if you have any questions - current fellows are ramping up to start this January and once we start, the fellowship is closed to new fellows until January 2026.
A very helpful blog for thinking in general.