

Exploring Causation and Diagnostic Accuracy (part two)
Thoughts about practice

In part one of this post I asserted that a good diagnostic test is built on causation and that measures of diagnostic accuracy are measures of correlation. Since correlation does not imply causation, but causation does imply correlation, it’s useful for us to consider the causal relationship between a diagnostic test and the condition it asserts to diagnose.
Part one:

Which was based on:

What we look for in a diagnostic test is that it is causally related to the condition it attempts to diagnose, but not as a cause of the condition. Rather as an effect of the condition. The factors that influence how good the correlation (diagnostic accuracy) is depends on mechanistic factors of causation including the presence of other causes. The condition we are attempting to diagnosis is the cause and the diagnostic test is the effect. It is important not to inverse this causal relationship. If we test something that causes a disease then it’s an etiological (another word for cause) or a risk factor. Its presence does not diagnosis the condition. Sometimes risk factors become diseases themself. Like elevated cholesterol. It was identified as a risk factor for coronary artery disease and cerebral vascular accidents and soon after it was considered a diagnosis in and of itself. The fact that the condition is the cause and the diagnostic test is the effect is an important consideration. It is the reason Bayes theorem and the resultant Bayesian inference is (at least subconsciously) utilized when interpreting a diagnostic test. In logical implication a cause takes the place of an antecedent and an effect takes the place of a consequent. Antecedent implies consequent. And if that is true, and you know the consequent is true, then saying the antecedent is true is literally a formal fallacy in logic called Affirming the Antecedent. Well, at least saying the antecedent is true on the basis of the consequent being true. I may revisit this in another post. It has been a while since I wrote about logic and causation - as I get back to writing I realize how much I miss it.
Back to causation and diagnostic accuracy.
The most important of Hill’s criteria for causation when considering the diagnostic accuracy of a test is specificity. The more specific the relationship between the test measurement and the diagnosis being tested, the stronger the diagnostic accuracy.
Specificity: Causation is likely if there is a very specific population at a specific site and disease with no other likely explanation. The more specific an association between a factor and an effect is, the bigger the probability of a causal relationship.

Even though Hill’s criteria is an epistemological system - a set of discussion topics to consider whether observational evidence justifies belief in a causal relationship - specificity is one topic that focuses on the ontology (the nature and being of the disease and the test (the system) under consideration).
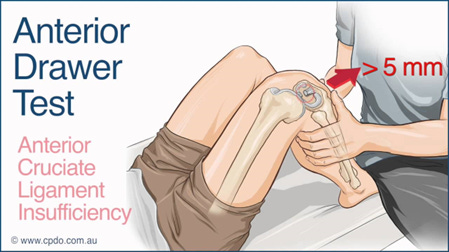
One of my held beliefs - something from the epistemology of critical realism - is that ontology determines epistemology. The nature of the system determines what we can know about the system (hence the challenges of quantum systems). Let’s consider the knee. As a system there are a few structures that prevent anterior translation (forward movement) of the tibia on the femur. These structures are the “being” of the system, the ontology. The Anterior Cruciate Ligament is the most impactful, followed by the hamstring muscles when they have increased tension (such as when “contracting”), and the joint capsule (relatively loose position when the knee is flexed between 15 and 90 degrees). The Anterior Drawer test of the knee is specific for diagnosing a torn Anterior Cruciate Ligament and its diagnostic accuracy measures (epistemology) are commensurate with the ontology. Factors that exist can lead to false test results. False test results can be false positives or false negatives. As a test for an ACL tear, false negatives are more common. Therefore this test tends to have higher specificity (0.78-0.98) than sensitivity (0.18-0.92) and better +LR than -LR (7, 0.5) , but has good diagnostic accuracy. Examples of factors that result in false results include joint hypermobility (false positives for diagnosing a tear), or false negatives caused by edema (expands and thus tightens the capsule and obscures visualization and feel of tibial translation), or hamstring contraction (since they are able to prevent anterior translation).
The point of this example is that consideration of the causal ontology helps us to consider the observation of diagnostic accuracy statistics. An ACL tear is very specifically related to anterior translation of the tibia on the femur and thus a positive Anterior Drawer test. The errors that create false positive or false negative results are related to the ability to accurately measure the phenomenon, as well as how specific the phenomenon is to the disease (or condition) we are attempting to diagnosis.
The same process can be performed for any other test. Some are straightforward because of ontological equivalence by definition. Hypoxemia is a blood oxygen saturation of less than 90%. This can be directly measured, so its accuracy is completely dependent on the accuracy of the measurement of the phenomenon. The measure IS the condition. They are ontologically equivalent. Therefore, for oxygen saturation measures diagnosing hypoxemia all we need to consider when considering diagnostic accuracy is measurement error. If we had a 100% accurate oxygen saturation monitor, then it would have 0 False Positives and 0 False Negatives for identifying the diagnosis of Hypoxemia, a Specificity of 100%, a Sensitivity of 100%. Another ontological equivalence by definition is Anemia. It is defined based on hematocrit levels. More challenging is the diagnosis of pulmonary or cardiac conditions based on hypoxemia or anemia. Hypoxemia and anemia have multiple causes, and therefore are not specific or sensitive to any particular cause (diagnosis). We can no more diagnosis heart failure based on hypoxemia than we can pneumonia; or bone marrow cancer based on anemia than we can an iron deficient diet. The point is - causation and ontology matter. Consider them when doing your examination and your evaluation, consider them when considering the diagnostic accuracy numbers of any particular “special” or diagnostic test.”
One more example from the world of orthopedic testing. The Crank test. It tests for the presence of a SLAP tear (superior labral anterior to posterior) in the glenohumeral joint (shoulder). It has a lot of reasons to be falsely positive or to be falsely negative and thus has a poor specificity and poor sensitivity, with poor +LR and -LR (1.33, 0.88). There are many reasons a tear will not create a click or catch, and there are many other conditions that will cause a click or a catch. If you use pain as the indication, there are even more problems that can cause pain during the Crank test movement.

As we started out - a good diagnostic test is built on causation and measures of diagnostic accuracy reflect the correlation that causation implies.
If you hold animosity towards the statistical processes for determining diagnostic accuracy then use them only as a guide to your interpretation of the ontology - the nature of the systems and the causal associations you’re testing with your examination tests. That’s all the diagnostic accuracy measures are anyway. They should not shake you from the clinical mechanistic reasoning about the anatomy, physiology, mechanics or pathology that drives and guides your reasoning process. Diagnostic accuracy statistics are guides, not replacements. And if that makes you feel overly subjective and not objective, then too bad. All things we hold to be objective are simply isolated parts of a much larger system for which we hold in our mind subjectively. The longer I have studied the pursuit of evidence for practice, the more I have come to realize that the best evidence for this objective pursuit is the story of its effectiveness, which is ontologically a subjective construct.